Why Midlife Hormonal Changes Are So Often Mistaken for Worsening Chronic Illness?
For many women living with chronic illness, there comes a point, often in the mid-thirties or early forties, when the body begins to change in ways that are difficult to explain. Symptoms that were once relatively stable may intensify. Fatigue deepens, pain increases, sleep becomes disrupted, and concentration falters. The immediate concern is often that an underlying disease is progressing. For women with autoimmune conditions, this fear is particularly acute. Yet in many cases another powerful biological transition is occurring at the same time: perimenopause, the hormonal stage that precedes menopause.
The challenge is that the symptoms of autoimmune disease and perimenopause overlap so closely that they are frequently mistaken for one another. Women may spend years believing their illness is worsening, adjusting medications or undergoing repeated investigations, when in fact changes in ovarian hormone production are significantly influencing immune activity, inflammation, and neurological function.
Understanding the relationship between the endocrine and immune systems is therefore essential, not only for accurate diagnosis but for improving the quality of care available to women navigating chronic illness in midlife.
Understanding Autoimmune Disease
Autoimmune diseases occur when the immune system mistakenly identifies healthy tissue as a threat and begins attacking the body’s own cells. Normally, immune responses are tightly regulated to distinguish between self and foreign pathogens. In autoimmune disorders, however, this regulatory mechanism becomes dysregulated, resulting in chronic inflammation and tissue damage.
More than eighty autoimmune conditions have been identified, including rheumatoid arthritis, systemic lupus erythematosus, multiple sclerosis, Hashimoto’s thyroiditis, inflammatory bowel disease, and psoriasis. A striking feature across this group of disorders is their disproportionate prevalence in women, who account for approximately three-quarters of all autoimmune cases. Researchers increasingly attribute this disparity in part to the influence of sex hormones on immune signalling pathways.
Although each autoimmune disease has distinct clinical features, many share common patterns of systemic inflammation. Individuals frequently experience persistent fatigue, musculoskeletal pain, cognitive difficulty often described as “brain fog,” fluctuating disease activity, and periods of exacerbation known as inflammatory flares. These flares can occur unpredictably and are often triggered by physiological stressors, infections, hormonal shifts, or environmental factors.
Management typically requires a combination of targeted medical therapies aimed at modulating immune activity and broader lifestyle strategies that support systemic health. Anti-inflammatory dietary patterns, restorative sleep, stress regulation, and carefully structured physical activity are commonly recommended to help reduce inflammatory burden and improve overall resilience.
Menopause and the Hormonal Transition
Menopause itself is defined clinically as the point at which a woman has experienced twelve consecutive months without menstruation, marking the end of reproductive capacity. However, the physiological transition leading to this point, known as perimenopause, is often far more symptomatic and complex.
Perimenopause may begin several years before menopause and in some women can start as early as the mid-thirties. During this period, ovarian hormone production becomes increasingly irregular. Oestrogen and progesterone levels fluctuate unpredictably before eventually declining, while changes in androgen levels also occur.
These hormonal shifts affect far more than reproductive function. Oestrogen receptors are widely distributed throughout the body, including in the brain, cardiovascular system, musculoskeletal tissues, and immune cells. As a result, hormonal fluctuations during perimenopause can influence neurological function, inflammatory pathways, thermoregulation, metabolism, and emotional regulation.
The clinical manifestations of this transition vary widely but often include disrupted sleep, mood variability, increased fatigue, cognitive changes, musculoskeletal discomfort, and altered stress tolerance. Many women also experience changes in libido, menstrual irregularity, and vasomotor symptoms such as hot flashes and night sweats. From a physiological perspective, perimenopause represents a period of systemic adaptation, during which the body recalibrates in response to shifting endocrine signals.
Why the Two Conditions Are So Often Confused
One of the most striking aspects of the menopausal transition is how closely its symptoms resemble those of autoimmune disease. The overlap occurs because both processes involve inflammatory signalling, neuroendocrine regulation, and immune system activity.
Oestrogen, for example, plays an important role in modulating immune responses. It influences cytokine production, regulates immune cell behaviour, and exerts anti-inflammatory effects in certain tissues. When oestrogen levels fluctuate dramatically, as they do during perimenopause, the balance of these regulatory processes can change.
For women already living with autoimmune disease, these hormonal fluctuations can alter symptom patterns and, in some cases, intensify inflammatory responses. The result is a clinical picture in which it becomes extremely difficult to distinguish between disease progression and hormonal transition.
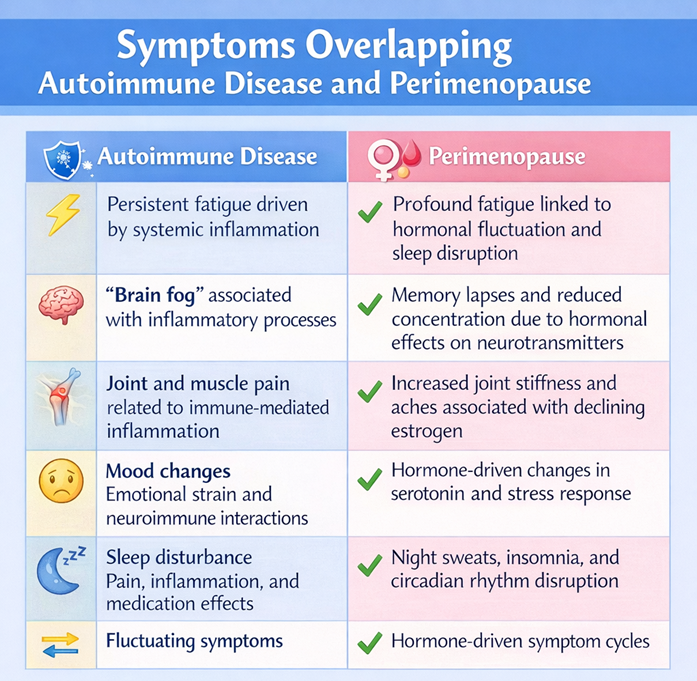
The similarities are particularly evident when examining the shared symptoms associated with both conditions.
The resemblance is so pronounced that many women struggle to identify which process is responsible for their symptoms.
The Particular Challenge for Women with Chronic Illness
For women already managing autoimmune or chronic inflammatory conditions, the interaction between hormonal cycles and immune activity is not new. Even during reproductive years, many patients report that their symptoms vary across the menstrual cycle. During the follicular phase, rising oestrogen levels often correspond with improved energy and reduced pain. In contrast, the luteal phase, characterised by progesterone dominance and declining oestrogen, can be associated with increased inflammation, heightened pain sensitivity, and emotional vulnerability.
When perimenopause begins, these cyclical patterns become less predictable. Hormone levels fluctuate more dramatically, and the stabilising rhythm of the menstrual cycle begins to break down. For women with chronic illness, this can result in more frequent or intense symptom fluctuations. Consequently, many patients experience what feels like a sudden deterioration in their health. Fatigue may become overwhelming, inflammatory pain may intensify, and cognitive symptoms may worsen. Without recognition of the hormonal context, these changes are easily interpreted as evidence that the underlying disease is progressing.
Yet emerging research suggests that the menopausal transition itself may represent a pro-inflammatory physiological state, which can interact with existing inflammatory disorders.
The Need for Greater Clinical Awareness
Despite the significant impact of hormonal transitions on chronic illness, many women report that perimenopause is rarely discussed during routine medical care until menopause is already well established. This gap is particularly concerning for women living with autoimmune disease or other chronic inflammatory conditions.
Greater clinical awareness is needed to ensure that hormonal transitions are considered when evaluating changes in symptom patterns after the age of thirty-five. Collaboration between rheumatologists, endocrinologists, and gynaecologists may be particularly valuable in these cases, allowing for a more integrated approach to care. When hormonal instability is identified as a contributing factor, treatment strategies may include both lifestyle interventions and medical therapies aimed at stabilising endocrine function.
Integrating Holistic and Medical Approaches
Many women understandably explore holistic approaches to support their health during hormonal transitions. Nutritional optimisation, stress-reduction practices, and botanical therapies such as adaptogenic herbs may help support resilience and overall wellbeing. However, it is equally important to recognise the role that evidence-based medical treatments can play, particularly for individuals experiencing severe perimenopausal symptoms.
Hormone replacement therapy (HRT), when prescribed appropriately, can stabilise fluctuating oestrogen levels and has been shown to improve sleep, cognitive function, vasomotor symptoms, and overall quality of life for many women. In the context of chronic illness, stabilising hormonal fluctuations may also reduce the severity of symptom exacerbations. Rather than viewing conventional medicine and holistic therapies as opposing approaches, many clinicians now advocate for integrative care models that combine the strengths of both.
Moving Forward: Supporting Women Through Midlife Health
The intersection of autoimmune disease and perimenopause represents an area where greater research, clinical awareness, and patient education are urgently needed. Women navigating chronic illness are already managing complex and often unpredictable health challenges. When hormonal transitions occur at the same time, the resulting physiological changes can feel overwhelming and deeply destabilising.
Recognising the profound similarities between autoimmune symptoms and perimenopausal changes is an important step toward improving care. For women over the age of thirty-five who experience sudden changes in health, exploring hormonal status alongside existing medical conditions may provide valuable insight.
Ultimately, supporting women through midlife health requires a more nuanced understanding of how hormones, immune function, and chronic disease interact. With better awareness, integrated care, and continued research, it becomes possible not only to manage symptoms more effectively but also to ensure that women receive the comprehensive support they deserve during this pivotal stage of life.
Medical Disclaimer:
The content provided in this educational material is for informational and educational purposes only. It is not intended as medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional regarding any medical concerns, symptoms, or conditions. Individual experiences with autoimmune diseases, perimenopause, or other health issues may vary. The creators and distributors of this content do not accept any responsibility for adverse outcomes or health-related decisions made based on the information presented.
References
- Desai MK, Brinton RD. Autoimmune disease in women: endocrine transition and risk across the lifespan. Front Endocrinol. 2019.
- Cutolo M et al. Estrogens and autoimmune diseases. Ann N Y Acad Sci. 2006.
- Gameiro C, Romão F. Menopause and aging: changes in the immune system. Maturitas. 2010.
- Sammaritano LR. Menopause in patients with autoimmune diseases. Autoimmun Rev. 2012.
- McCarthy M, Raval AP. The peri-menopause as a systemic inflammatory phase. Journal of Neuroinflammation. 2020.
- Cutolo M et al. The impact of menopause on autoimmune and rheumatic diseases. 2024 review.
- The Menopause Society. Hormone therapy and autoimmune disease risk. 2025.
- Hermann T. How perimenopause affects immunity.
- Winona Health. The link between menopause and autoimmune disease.





